Blog
Software-defined medical devices are evolving
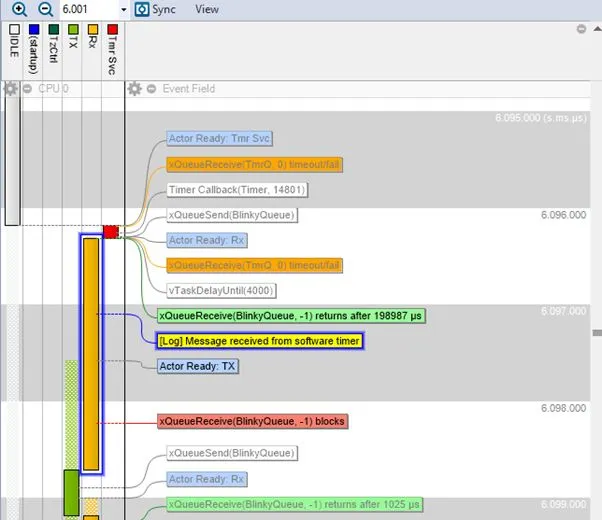
The trace view shows the runtime behaviour of a real-time system, including task scheduling, interrupts and concurrency, making temporal dependencies visible. Pic: Percepio AB
The medical device industry is entering a transition that, while less visible than the automotive shift to software-defined vehicles, may prove just as consequential. This transformation is being enabled by a new generation of ultra-low-power, high-performance hardware platforms. Devices are no longer limited to simple sensing and transmission. They increasingly support continuous monitoring, local data processing and even on-device inference – all within tight energy, safety, and real-time constraints.
At first glance this appears to be a straightforward story of technological progress. In reality it introduces a new and underappreciated challenge: a rapid escalation in system complexity at the very edge of regulated, safety-critical environments.
Complexity moves to the edge
Much of the complexity in digital health systems has resided in backend infrastructure – cloud platforms, analytics pipelines and clinical software systems. Edge devices were comparatively simple, often acting as data collectors rather than decision-makers. That boundary is now shifting.
Modern medical devices are expected to:
- Continuously acquire and process physiological signals
- Maintain reliable wireless connectivity
- Execute increasingly sophisticated algorithms
- Operate for extended periods on constrained power budgets.
These requirements are driving adoption of real-time operating systems such as Zephyr RTOS and higher-integrity alternatives used in safety-critical systems, including SAFERTOS. They are also accelerating the move towards multi-threaded, real-time software architectures.
As a result the kinds of problems engineers face are changing: issues no longer arise solely from incorrect logic within a single function. They emerge from:
- Timing interactions between concurrent tasks
- Resource contention under varying workloads
- Subtle race conditions that only appear in real-world operation.
In other words the edge is becoming a distributed, real-time system in its own right – one that must operate deterministically under all conditions relevant to patient safety.
The visibility gap
In many industries increasing complexity is addressed through better tooling, faster iteration and continuous integration practices. In medical technology, however, there is an additional dimension: the need to demonstrate correct and safe behaviour through objective, verifiable evidence.
Traditional debugging methods – breakpoints, logging, post-mortem analysis – were not designed for this level of concurrency, nor for systems that cannot easily be paused, reproduced, or instrumented without side effects. More importantly they do not provide the kind of objective runtime evidence required in regulated environments. This creates a visibility gap.
Engineers may be able to infer that a system behaves correctly under certain conditions, but inference is not the same as verifiable behavioural data. In a regulatory context it is evidence that underpins validation, traceability and, ultimately, trust.
From debugging to evidence
As systems become software-defined and real-time behaviour becomes central to their function, observability evolves from a debugging aid into a foundational capability.
Observability, in this context, is not about collecting more logs. It is about gaining continuous, low-overhead insight into how a system behaves during actual operation:
- How tasks are scheduled and executed
- How timing constraints are met – or missed
- How different components interact under load.
For companies developing software-defined medical devices this kind of insight serves multiple purposes. It helps engineers to identify and resolve complex system-level issues more efficiently. It strengthens verification and validation by providing objective, fine-grained evidence of how the system behaves under realistic conditions. It extends beyond development, supporting confidence in system behaviour during real-world use after deployment.
This is not a theoretical shift. Across safety-critical embedded domains the growing importance of understanding actual runtime behaviour has already driven the adoption of more advanced observability practices. In systems built on high-integrity real-time operating systems such as SAFERTOS, deterministic behaviour and verifiable execution are not optional – they are essential requirements.
Many of the world’s leading medical technology companies are now encountering the same class of challenges: increasing software complexity, non-deterministic timing behaviour and the need to demonstrate system performance under real-world operating conditions.
A different trajectory
There are clear parallels between this evolution in medical technology and the rise of the software-defined vehicle. In both domains software complexity is expanding rapidly and traditional development approaches are reaching their limits.
However, there is also a critical difference. In automotive the primary driver for adopting observability has been scalability – enabling teams to manage increasingly complex systems and accelerate development cycles.
In medical technology the driver is more fundamental: complexity, safety and evidence requirements converge in the same place. Systems must not only function correctly, but their behaviour must be understood, documented and defensible in a regulatory context.
This distinction has important implications. It suggests that observability in medical devices will not simply follow the same adoption curve as in automotive. Instead, it is likely to become embedded more deeply into development, validation and lifecycle management processes – precisely because it addresses both engineering and regulatory demands.
Looking forward
The evolution of software-defined medical devices is not happening in isolation. It is being driven by broader shifts in healthcare delivery and demographics. Ageing populations, the rising prevalence of chronic disease and increasing pressure on healthcare systems are accelerating the move toward home-based care, outpatient treatment and continuous remote monitoring.
In this context medical devices are no longer occasional diagnostic tools. They are becoming persistent, software-driven systems that operate continuously, often outside controlled clinical environments, and increasingly closer to the patient.
At the same time more intelligence is moving into the device itself. Advanced algorithms and on-device AI are enabling new forms of real-time analysis and decision support at the edge. But as systems become more autonomous and inference-driven their behaviour becomes more complex and less directly observable. This amplifies a fundamental challenge: understanding not just what a system is designed to do, but how it actually behaves in practice under real-world conditions.
With these shifts the need for visibility is no longer limited to engineering efficiency. It becomes central to safety, validation and trust. It is no longer sufficient to design systems that are intended to behave correctly. It becomes necessary to demonstrate, with precision, how they behave in operation – across all relevant conditions and over time.
This is the direction in which software-defined medical devices are heading. Continuous observability is therefore not simply a technical enhancement, but a core capability – supporting not only better engineering, but also the evidence, transparency and confidence required to scale healthcare beyond traditional clinical settings.
In software-defined medicine what cannot be observed cannot be evidenced. And what cannot be evidenced cannot be trusted.
See: Safety and compliance innovation in medical equipment